Parents aren't passive consumers of care. We teach you what you're looking at.
The words your pediatrician uses
TM. AOM. OME. Bulging. Watchful waiting. Knowing the words means you can read the plan and ask the right questions.
What ear-infection findings look like
Normal vs. bulging vs. obscured. We show you what a clinician is looking for and what counts as a real finding vs. an inconclusive view.
What raises a child's odds
Age, daycare, smoke exposure, family history, season. Knowing the risk profile means you understand why a recommendation is what it is.
01 Vocabulary — words your pediatrician uses
| Term | What it means |
|---|---|
| Tympanic membrane (TM) | The eardrum — the thin barrier at the end of the ear canal. |
| Acute otitis media (AOM) | Middle-ear infection with fluid and inflammation; the condition most people mean by "ear infection." |
| Otitis media with effusion (OME) | Fluid behind the eardrum without acute infection signs. Common after AOM; usually doesn't need antibiotics. |
| Bulging | The eardrum pushed outward by fluid or pus — a core AAP criterion for diagnosing AOM. |
| Watchful waiting | AAP-endorsed approach: in selected non-severe cases, observation for 48–72 hours before starting antibiotics. |
02 Images — three things a pediatrician looks for


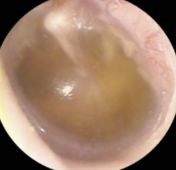
Otoscopy images provided by EarRx clinical team.
03 Risk factors — what raises a child's odds
Age under 2
Anatomy and immune development both push incidence higher in this window.
Daycare attendance
More respiratory viruses in, more otitis media out.
Tobacco smoke exposure
Secondhand smoke is a well-documented modifiable risk factor.
Bottle-feeding while lying down
Positioning affects eustachian-tube drainage; feeding upright helps.
Family history
Recurrent AOM runs in families. We ask about it in the intake.
Seasonality
Rates rise with the winter respiratory-virus season.



